
Foundational Statements that guide my approach to intervention in the ASD microbiome
Author Bio

I’d like to start by introducing some statements as a foundation that I will revisit. In some cases these are the principles that guide my approach and understanding of intervention in the ASD microbiome. These are formed from my experiences and are solely my opinion on the matter. I welcome the discussion surrounding them.
1. Given two different individuals, if we could impart the same change in microbiome status (improvement) it can cause two considerably different levels of clinical improvement, also given two individuals, if we could impart the same dysbiosis to each of them it would impart potentially two different insults to their ability to function, this is because the functional state of the individual is only partly dependent on the microbiome but also dependent on other toxicities or issues present at that moment. Furthermore, even small improvements in the biome (as we can measure) can provide substantial clinical improvements. The act of removing toxicity negatively affects the body and the microbiome, it is inevitable but there are tools to support it .
2. Prescriptive components are powerhouses that disturb the balance, and their mode of action is often beyond what is advertised. (Antifungals affect bacteria too and vice versa). Don’t think that pharmaceuticals or herbs act in a silo, pharmaceuticals are extremely potent and focused agents and should be assumed to affect balance unless otherwise proven. The continuous administration of a pharmaceutical can also tip the balance unless there is action taken to remediate that impact.
One needs to limit as much as possible the use of antibiotics, antifungals and even antivirals for treatment, at the very least in their continued use. There are other pathways that are more sparing of the Gut Ecosystem, if these prescriptives are needed one should at least first consider the herbal alternatives which are often less focused and/or options of Pulsing and followed by alternative prebiotic / probiotic intervention to mitigate the damage caused. There are practitioners that treat for instance PANS and PANDAS with the regular use of antibiotics and other prescriptives and they advertise these as Treatment Protocols, often time chasing improvements which are followed by exacerbation of other issues. I completely and fundamentally disagree with this approach. From the perspective of a parent who saw significant benefits with antibiotics and even antifungals- one needs to always ask what is the timescale for assessment for these particular therapeutics, if we are only evaluating the immediate gains and not the damage that appears much later then are we missing the big picture. What we gained very quickly was lost over months and created fungal states that were unimaginable. I don’t like stating absolutes, but I believe Practitioners should not be using antibiotics to treat autism. Antibiotics are often an instigator or contribution for regression. Prescriptives need to be taken with caution, pause, and a well-thought-out strategy if needed at all. I have learned this the long and hard way, and I’m prepared to argue these points vehemently.
Another misunderstanding is the dominant “killing” action when taking a prescriptive (antibiotic, antifungal, etc). The thought is that these drugs are causing or are responsible for fighting the target pathogen, in actuality the dominant process of killing (in a healthy person) occurs from antibodies formed from antigens after the initial “kill” event. Your immune system rallies against the debris left from the initial kill. Such is the case that the same therapeutic can cause two different responses based on the state of the immune system. For instance the diflucan “Kill” in a healthy biome will be more effective than the “diflucan Kill” in a weaker biome. So my argument is not only should you try to minimize these prescriptives for their effects on the biome, but if you do consider them, they will have a better effect once the biome is in a better place,and pulsing, I believe, is most often a better choice if warranted at all. We know from the studies on oncologic patients that those who received immunotherapy and were initially non-responders became responders after initiating FMT and repeating the immunotherapy treatment. My argument is you must strive to harness your immune system to your side and by bringing your biome away from the extremes you can obtain this benefit.
3. We need to understand that the gut is a primary mode of evacuation of toxicity in the body, and that in itself might be the reason for the perpetual battle of dysbiosis in some, as the systemic toxicity can act as a forcing function which requires that you have your finger on the button of microbial intervention for some time, months to years with gradual improvements. Toxicity exists in various forms, past exposure, present external exposures and burdens from within. Many people don’t realize that the Microbes find a way to break down what is in you (for good and bad). For instance, a popular laxative that includes polyethylene glycol was thought to be safe on basis that humans do not have the enzymes to break this compound down….. However no one ever looked at whether bacteria could do so. The product of the degradation is ethylene glycol (ANTIFREEZE).
4. Don’t bet on one hit wonder solutions to “fix the issue” particularly in the GUT, for instance FMT - these can be very random gambles regardless of the donor quality, they can initiate MCAS if you have the conditions are right. The healing sometimes isn’t meant to be quick, it is a lengthy process and even FMT when successful will almost certainly require continuous feeding / intervention because the problem isn’t always in the gut, it is just that the gut takes a direct beating when detoxifying". I have witnessed enough FMT cases gone awry, and some that were “successful” fall backward. My focus is on feasible and practical solutions, FMT may be something that can fall into that category one day and I love the connections and amazing stories of improvement that have been documented.
At the current moment if you were looking for the benefits of FMT, I believe that finding and screening a healthy toddler family member is better than anything practitioners can provide, cheaper, and feasibly re-doable (rectally), despite this I think Gut Balancing is a better and ultimately inevitable necessity.
5. Perfection is the enemy of progress, your protocols need to be broad but flexible. Your diet needs to be broad but forgiving, abstaining from everything that is classified as bad can be impractical and knock down the entire house of cards. For instance individuals will completely cut out fruits because of the sugar content. It is the processed foods that we want to avoid, minimize things that cause strife, and broadly eat many things without binging, keeping moderation in mind. Eating fruit isn’t the reason why you have inescapable fungal overgrowth, and abstaining from eating it isn’t going to be the reason why it goes away either. Similarly the ideologies of removing anything related to or has been used in the same sentence with glutamate, or carving out every oxalate from your diet is a rash protocol. You might see some benefits but for the class of individual that is moderate to severe you will often sacrifice other benefits to hold these abstinences. There is also a time evolution for these ideas. For instance, excluding dairy may be an appropriate tool to reduce inflammation and prevent molecules from leaking across hyperpermeable mucosa, but as you heal, there is a place to include some dairy. In other words there is a benefit (many lactobacillus feed on dairy strong compounds) in including some dairy as you are able to tolerate it. (I recommend looking at Goat / Sheep Milk cheeses).
6. Use the test to guide you, but just because you tested positive for something does not mean that is the reason for your health issues, oftentimes it is a feature but not the origin or the place to start, this is very true with fungal overgrowths, including Mold colonization. The presence of abnormalities on tests could be features of other issues, and if you are only focused on normalizing a test, then you can lose sight of what may be important. I have done enough of these tests, some several in the same day to get an appreciation on their variability in part due to the inherent variation in the body at that moment. Understand that many test values can also fluctuate or require certain conditions for you to actually make comparable measurements over time.
7. Reaction and reactivity do not indicate inappropriateness, quite the opposite. I have scores of people that have told me that they can not take X, Y, or Z because they experience reactions from those items. This topic is heavily discussed in the realm of histamine and is severely misunderstood. Simply put, if you took these things in the past without issue and or if you take them and your reactions diminish with time, the reaction and reactivity you are experiencing is the product of your dysbiosis and shifting in the biome. I will touch on this more later.
8. If the protocol you are attempting is not practical or feasible or forgiving (requires perfection), then it is not a protocol worthy of trying.
9. Don’t discount genetics but don’t let them rule your fate. The number of gene encoding enzymes by the microbes in your gut is enormous. Metagenomic study of the human microbiome has demonstrated that there are 3+ million unique genes in the human gut, ~150 times more genes than our own genome. If you're using your DNA snps to corner yourself into what you should and shouldn’t take - keep in mind there is a microbial voice that is just as powerful as you may be forgetting about. In my experience those that treat solely based on genetic snp-s limit themselves, if they were the cause of your issue then we wouldn’t be able to explain regressions, or changes in function at later stages in life, spark events, etc. I’ve met practitioners that want to show me these exotic genetic tests, not realizing I’ve already extensively researched and performed several times over said testing…and the clinical intervention based on that produces limited results on their own. Genetics play a role much like your hand in a game of poker but rarely play the extreme limiting role that many make them out to be. There are a lot of fancy expensive Genetic tests out there, in my experience tweaking on genetics only gets you so far.
10. Don’t pin all of your problems on the dysbiosis in your gut. I do think dysfunction in the gut can be the impetus in many situations for the house of cards to fall down, I also believe it can be a slower contributor that builds up with time or even a spark like event when insulted, I believe the Gut status can be the product of some other trigger event as well. However if we only focus on the gut we lose sight of the complexity and interconnectedness of the issues that prolong, contribute, and initiate disease.
11. Bacteria, Yeast, Mold, Virus, Parasites, Heavy Metals, Lyme, Autoimmunity, Malabsorption, Mitochondrial dysfunction, Pans, Pandas, Is this really what is going on? You stumble upon an abandoned home, it appears the home had fire damage, water damage, and animal inhabitants. Which of these things happened first? Was it roof damage that caused the leaks and water damage, then creating an electrical fire in the home followed by the vacancy of the owners, termite and animal inhabitants. Could it have been the fire that started first, causing damage to the roof and so on. Is it possible that the termite problem was so bad that the owners left, leaving the house vacant and subject to the elements, leak, electrical fire etc. Could lightning have struck this ungrounded home causing a fire, etc. The point that I’m illustrating is that if you are looking at the end product of dysfunction, there are many ways to get there so its impossible to answer the question what was the cause.. There are certainly contributions to the current state and they superimpose and feedback, perpetuating the dysfunction. You can’t fix the home without fixing the roof, treating the termites and water damage, etc. What is the best order to fix the home? What we know is that the microbiome balance is tied to the state of microbes, ,fungi, protozoa, detoxification of toxicity including heavy metals, immune function, autoimmunity, intestinal permeability, malabsorption, inflammation, metabolism, etc. etc. We shouldn’t take from this that it all starts in the gut but we should understand that there are a lot of knobs that can be turned by tweaking the gut.
12. For those that are looking for that specific overgrowth or undergrowth of a species as the reason for their disease state I would boldly suggest that they instead look at the overall balance and try to connect the deeper reasoning as to why that overgrowth or undergrowth is present in the first place, don’t attempt to pin the problem on 1 item. There are many that pin the problem on (take a card) Klebsiella, Akkermansia, Methanobrevibacter, Clostridium, Streptococcus, etc. It must be understood that these do not exist in a vacuum and the human condition is to look for the bad guy, strike out what is wrong without analyzing the potential origins for those issues. Rats crowd the streets of NYC because there is a high density of people and trash available as food to feast on, it also happens with a cyclic natures (on the eve of garbage day). Termites infest a home because of the type of wood and sometimes the moisture content. For instance, In the case of the microbiome, Bifidobacterium plays a significant role in Gut PH. PH sets the climate for certain microbes to thrive much like growing conditions needed for various plants across the globe. We must understand the importance of balance in the microbiome not just targeting what is perceived bad or wrong (cut it out approach) and the relationship that this balance plays with the rest of the body, metabolism, genetics, detoxification, and neurotransmitter function.
13. Take advantage of the history and knowledge of therapeutics with centuries of use in treating ailments.
Before there was testing, in the age of the healer we had remedies for various ailments. In each civilization there are holy grail herbs, Chamomile, Triphala, Codonopsis (dan sheng), Mastica, Turmeric, Fennel, Ginseng, many more than I have listed here. These have the benefit of hundreds of years of use, there is valuable information and therapeutic potential in harnessing these when appropriate.
14. We must be aware of the timescale to assess improvement. If you are expecting to take something and see benefits in the same day, that is entirely possible with components that support metabolic function, most biome interventions require weeks, and oftentimes you will feel worse upfront. If you are expecting to take something and NOT see reaction and reactivity when dysbiosis is present, then you’ve been lied to. I would argue that if you're not seeing these exacerbations then you're not hitting the bees nest. Don’t specifically look for the probiotic you can tolerate. You should expect that the reaction and reactivity will dampen with time, and there are smart ways to support the reaction and reactivity including histamine suppressors, inflammation mitigation, pulsing treatment, antioxidants etc..
Here are two images that can help summarize the experience and the
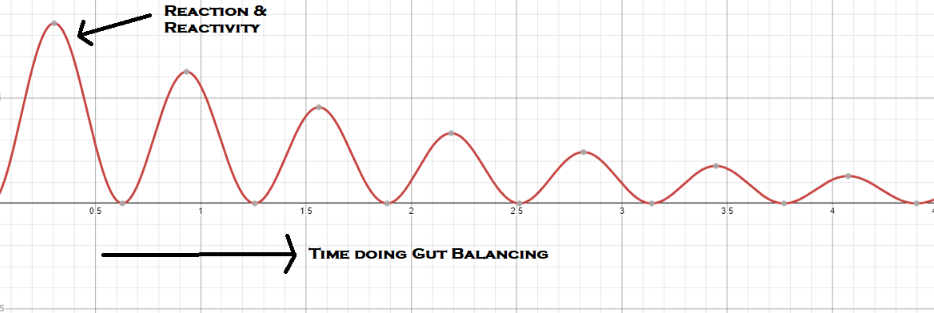
What is the timescale to assess change / improvement?

15. People ask about the role of the diet. I have specifically worked with many individuals that actually have some of the cleanest diets, full of all the ideal things to eat with it seeming to have little representation with respect to the test results. In other cases (quite common) there are significant overgrowths like Prevotella that align with certain diets (for instance mediterranean diet), despite the child or individual eating absolutely nothing from that type of diet. The clearest example is the 8 month and 18 month biomes where these children has not even introduced solids yet but have prevotella copri occupying some 50%+ of their biomes (and they live in mold conditions). As I stated earlier there are forcing functions that exist that perpetuate the dysbiosis, this can include fungal overgrowths that feed bacteria via their metabolites to systemic toxicity that dumps into the biome disrupting balance to even complex viral relationships with phages. The diet is important, but with extreme dysbiosis it takes a backseat almost always.
16. Along the same lines I will often hear the argument that biome balance various geographically, then how do we know what is ideal?
My counter argument is that no one has shown you can’t optimize your biome to be a healthy, Japanese biome, or Chinese, biome, or Greek biome, or Russian biome, etc. The goal isn't to balance your biome based on where you lineage is from or even based on your current diet or your mom’s cooking, it is to bring it away from the extremes found in the population. Regardless of the differences. There are still things each culture agrees upon (normal and extremes), it's that intersection that I argue (the guy in the middle is the safe place where you want to be) with respect to the microbiome. There will always be variation but there are clearly things that are not normal, typical. The “guy in the middle” is not necessarily the healthiest place to be but in the case of dysbiosis it's less unhealthy than in the extremes.
17. ASD is a broad diagnosis; the word potentially means something different for many. ASD is touted to be both medically based, yet it isn’t diagnosed as a medical disorder, often diagnosed by psychologists, psychiatrists, developmental pediatricians. There is an entire business model built around the diagnosis, insurance models to obtain and inhibit needed services. The definitions vary state to state, country to country. There are also those that align with the condition on the platform of neurodivergence. Surely this complicates anyone being able to discuss or talk about the same thing, even at the research level. This is why having only double blinded studies as the preferred study type is one of the silliest things particularly in the landscape of ASD. Somewhere we got the idea that we should let the placebo effect govern our research. I urge everyone to actually research the placebo effect, but this is besides the point. The correct way to assess clinical utility is by providing a placebo to the same individual, then giving that same individual the disguised therapeutic (blinded) and assessing outcome over time. Instead these studies are often performed giving the placebo to 25 people and the therapeutic to 25 different people and seeing which group does better. The latter assumes the people have the same dysfunctions and are a homogeneous group, this certainly is less true in ASD. In ASD more than any other group we have a heterogeneous population described by a word diagnosed by someone observing behaviors tied to therapy and services with extremely blurred boundaries. This is not to say these individuals are not autistic, but we can not pool them together and do research on them without determining commonality in their ailment. If you talk to any scientist (that does research and publishes in a physical science) you will realize that the ability to measure anything requires controlling the variables, if you can not assume the population is homogeneous then the utility is impaired, this is why if you want to correctly study a therapeutic and you are concerned about placebo you should initiate placebo then switch to therapeutic in the same group and NOT compare two different groups placebo vs therapeutic. I firmly believe this is why much of the literature published on ASD (or even outside this condition sometimes) has found conflicting data. Lastly the results of studies can be misleading and still include intended bias, studies cost money and require conformance to IRB’s and extraneous rules, we lack thousands of studies on therapeutics that are known to have benefits because they are not feasible or profitable to do. The only groups that can perform studies at will are those with money because they are insanely expensive because of the governance around them. At the end of the day studies are nice to have, must be taken with a grain of salt because the best metrics will always be what you can do with the patient and in your clinic, the origins of medicine did not initiate with an IRB, the randomization for placebo, or the interest of pharmaceutical development and sale, the healer was integral and harmonious with the patient without disconnect, the only goal was making the patient better.
That being said, the way that I classify the type of ASD that I work with is moderate to severe dysfunction in the following areas, gross and or fine motor coordination, identifiable GI issues, receptive and expressive communication, metabolic and or mitochondrial dysfunction, autoimmunity, dysautonomia.
18. When dysbiosis is present, your program must have broad action, redundancy, support, but also be flexible if you leave something out or can not access it. Typically those participating in GUT Balancing may require between 10 herbal pieces, 2 to 4 probiotics pieces, 1 to 3 antifungal pieces, 1 to 3 prebiotic pieces, and several pieces for support of various modes of dysfunction (histamine, oxalates, ammonia, adrenal, etc.). This means a very complicated program. The majority of those participating in gut balancing were doing so with about 15 to 25 different supplements, this is the reason why I designed our products available at ResearchedElements.com, along with Dr. Christian Bogner; they are meant to fill the common core, make participation more feasible, affordable, and practical. These components along with emphasis in certain areas (per test results) reduce the complexity and quantity of components needed to participate.
19. Don’t take probiotics expecting them to join your biome - assume that they do not colonize. Probiotics can shift balance in the gut, they typically act like sell swords, they go in and “police” and leave. Appropriate Prebiotics can be of the most powerful tools for shaping the gut including growth of the “good” and balancing where there is deficit, but it requires the knowledge of what is needed to be fed and how to feed it. Herbs play a similar role to probiotics in damping down sometimes with prebiotic effects too. The combination of all three are required to shape the gut when dysbiosis is present. If probiotics are the police in society, just having police will not solve the crime issues, you need stable jobs, economy, education, tourism, a legal system, etc. These are the roles filled by diet, prebiotics, herbs, etc., the tools we have to get things back in order.
20. Wait, I have parasites, Mold, MCAS, Phenol Sensitivity, Salicylate Sensitivity, Copper Imbalance, heavy metals, Lyme, bartonella, fungal overgrowth. I need to treat these things first before working on the gut? No!, I would say you want to start with the gut, the sensitivities you will find will diminish with time, and you will gain a better immune function so that other treatments you pursue will have a higher chance of success. Phenolic compounds and salicylates are ubiquitous in foods such as fruits and vegetables. Often times the reason for people's reactions to them is their gut status, when you properly intervene there and support your body those reactions and reactivities diminish. For almost every individual that I have encountered in the adult world with these sensitivities and intolerances, they had no problem eating them before their “event”. If you have eaten these things in the past without issue, the status of the microbiome / mucosa is very likely the culprit. No one is saying to binge on these items that are reactive, but critical abstaining when the compound that has other benefits will perpetuate your feedback loop. At the end of the day practical moderation is a good rule to apply.
21. I have SIBO, I have Candida, I have Mold. These are common statements that I hear and I would say the vast majority of people have their own diagnosis wrong, I’m not disputing the existence of these situations however many of these catch words can funnel you down the wrong paths. I would estimate that more than half that believe they have SIBO don’t seem to have the classical overgrowths that accompany them - we must not assume that when you have reaction and reactivity to taking things that you have SIBO. No one is doubting your pain or discomfort. Regardless, I find it less productive to discuss these points and just incorporate components that will address the issue even if it was there. It is important to distinguish that if you believe you have SIBO, that isn’t a contraindication for probiotics - remember probiotics won’t colonize, they will damp down overgrowths and are very appropriate in these cases. SIBO can actually be thought of as a deficit in some ways of beneficial microbes. Regarding the Candida and Mold statements, keep in mind that molds do naturally occur in the gut, so surely you mean you have a non-ideal overgrowth of MOLD. Candida is a genus for which there are several species for, it is quite vague and likely you are inferring this from some indirect method (which is fine). There are no great tests for fungi, ITS testing can offer some ways to measure the fungal problem but we are limited with fungal libraries, the complexity that the fungal ITS gene is quite variable in base pair length (unlike the 16s gene) and even if you found the problem would you actually have more actionable information to do something different about it other than what you would do with a standard clinical approach. Remember the interventions for fungal overgrowth don’t really change depending on what you may have found. Back to the MOLD quantification issue… the best way to term this entire issue is fungal overgrowth. MOLD is not the same as elevated mycotoxins, mycotoxins can also be produced from yeasts (candida) growing inside you, or you could be exposed as well. There are a lot of thin lines here and the distinctions don’t necessarily make a difference. We can not pin the entirety of fungal problems on Candida and Mold solely. There are many yeasts that can actually behave like molds in different PH environments. At the end of the day I argue that the intervention to address these things looks similar, it must be feasible and practical and it must be supportive of the biome.
22. I need a stool test that tests for “pathogenic species” so I can know if I have them or not. You should always ask the question, “is the test going to actually dictate how I treat the issue, will it affect my intervention?” If an individual has elevated proteobacteria or a specific identified proteobacteria I will still approach that component the same way clinically, with broad targeting and support for the beneficial microbes in the gut that will lock in defense. You might say but why would you want to limit yourself to not knowing what is really growing, and my response would be
-
What's the point of trying to determine what's wrong with the house if it's currently on fire?
-
I’m trying to not send this patient to the poor house by suggesting testing that won’t change the intervention. I include a broad component to cover this and believe that work done to restore balance will further the effort.
In the case of bacteria/archaea, The majority of pathogenic microbes can be pooled into the phylum of proteobacteria and luckily there are many tools that provide broad assistance with targeting proteobacteria. (I like Pomegranate Peel as one of them). Also know that their presence will often be a function of your GUT Climate (PH) and lack of beneficial microbes and or chronic or stored toxicity. Remember that tests that use only qPCR techniques to look for lab suggested issues, will only be able to find those and may miss items, they are also subjected to their in house ranges and you can not compute relative abundances in qPCR.
23. What about heavy metals where do they stand in this? If you have listened to some experts like Dr. Chris Shade, the individuals that ‘got good at working the gut’ have seen progress in the heavy metal arena, that is because you can accumulate toxicity (including heavy metals) if your biome is not balanced for different reasons, 1) microbes play a role in detoxification, 2) if you gut is permeable that adds a burden to detox and can allow leaking to happen, 3) if you gut is inflamed that takes away energy and detox power to deal with the daily exposures you face, LPS etc. The biliary system is implicated heavily in detoxification, there is a feedback loop between gut / liver / brain.
24. What about binders? You can get very fancy, there are dozens of binders out there and then you will find a practitioner that tells you to time the binder relative to taking a probiotic or herb. I strongly feel that your program must be feasible and practical, if you make it too complex then things start to fall apart. I prefer to use a simple good quality activated charcoal and I’d rather take it a few days per week and before bed assuming that constipation is not an issue. Activated charcoal is one of the safest binders and has an affinity for many things, it's a great endotoxin binder.
25. There are many that don’t believe that the Autism Gut is any different from the Neurotypical Gut. When you have heterogeneous populations and broad definitions of the disorder, I’m surprised people could come to this conclusion. Who cares… There is dysbiosis in and outside of autism, the correct position should not be comparing the ASD gut to the non ASD gut, the position should be…. there is clearly improvement seen when you intervene in the ASD Gut, it is a tool for modulating health, detoxification, metabolism, etc. There are claims that the microbial state is a product of the diet / picky eating. I have seen personally some of the cleanest diets in ASD still yield and perpetuate dysbiosis, I have also seen diets that do not reflect their stated microbial signatures like in the case of Prevotella copri (the 8 month old who has a 55% abundance of this microbe who somehow has embraced the Mediteranean diet). There are a lot of people ready to write off what is and what isn’t, particularly those haven’t been privy to the experience of improvements in ASD by modulation of the gut.
26. “My son can not take these things, he is allergic to anything red and purple (fruits / veggies).” No your son is not allergic to colors, after verifying this via email exchange, the issue is the child is reactive to polyphenols because.
-
He has intestinal permeability
-
He has dysbiosis that responds to these polyphenols and causes reaction and reactivity
The word allergy when used in the context of food should be delineated from an intolerance, allergies produce anaphylactic reactions and are IgE-mediated, meaning that IgE-allergy antibodies are a cause of the allergic reaction. IgE-mediated food allergies usually occur within minutes of ingestion and include hives, redness of the skin, vomiting and in more severe reactions, anaphylaxis. There are other antibodies IgA, IgM, IgG each with their distinct immune relationships, IgG tests are commonly emphasized for food reactivity / sensitivity but this kind of testing is widely variable depending on the status of intestinal permeability. In other words, IgG testing can be misleading in the presence of dysbiosis and does not reflect a true Allergy. I have seen IgG testing improve after working the microbiome, I have also seen the reaction and reactivity indicated above diminish with GUT intervention and over time. I find the “food allergy” tests to be of little to no utility, the word allergy should not be used in those tests as it is misleading.
27. “My child has Clostridia, I can tell from his OAT test and his symptoms”. Clostridia is a Class of Bacteria, there is a hierarchy in the phylogenetic tree, Domain kingdom phylum class order family genus species, strain. If you were to look at a sample of a thousand people, you find that the majority of people have Clostridia (a class) occupying 40 to 60% of their entire microbiome. If Clostridia is pathogenic that sounds weird that it takes up half of our biome? Well the infamous OAT test that looks for markers associated with Clostridia is a bit misleading.
-
They are mistakenly using the word Clostridia to mean the plural of Clostridium.
-
If you speak to their founding expert, he has admitted to me that the microbes that they have associated with elevations in organic acids are SOME of the microbes that produce those organic acids but they are not ALL of the microbes that produce those organic acids. Don’t get me wrong, having elevated HPHPA for instance is non ideal and neurotoxic but it does not mean that you 100% have a Clostridium overgrowth (which they are incorrectly calling Clostridia).
-
The other complication to this discussion point is that the grouping of many Clostridium have changed over the years and labs that do not keep up with these NCBI characterizations may be incorrectly identifying the same microbes. For instance below is just a small list of [Clostridium] That have been redefined out of that Genus, they are no longer considered Clostridium. If you are not compliant with following NCBI naming then you are potentially confusing or misleading people.
[Clostridium] aldenense → Enterocloster
[Clostridium] alkalicellulosi → Acetivibrio
[Clostridium] aminophilum → Lachnoclostridium
[Clostridium] cellulolyticum → Ruminiclostridium
[Clostridium] citroniae → Enterocloster
[Clostridium] cocleatum → Thomasclavelia
[Clostridium] colinum → Tyzzerella
[Clostridium] glycyrrhizinilyticum → Mediterraneibacter
[Clostridium] hylemonae → Lachnoclostridium
[Clostridium] innocuum → Thomasclavelia
[Clostridium] lactatifermentans → Anaerotignum
[Clostridium] leptum → Oscillospiraceae incertae sedis
[Clostridium] methylpentosum → Oscillospiraceae incertae sedis
[Clostridium] polysaccharolyticum → Lachnoclostridium
[Clostridium] scindens → Lachnoclostridium
[Clostridium] spiroforme → Thomasclavelia
[Clostridium] sporosphaeroides → Oscillospiraceae incertae sedis
[Clostridium] sporosphaeroides → Oscillospiraceae incertae sedis
[Clostridium] stercorarium → Thermoclostridium
[Clostridium] symbiosum → Lachnoclostridium
[Clostridium] viride → Oscillospiraceae incertae sedis
[Clostridium] citroniae → Enterocloster
[Clostridium] lactatifermentans → Anaerotignum
[Clostridium] histolytica → Hathewaya
[Clostridium] bolteae → Enterocloster
Don’t get me wrong, those OAT tests can be helpful but microbial testing like 16s will always provide more overall information, whereas the OAT is more complimentary.