
Broad Guide For Intervention in Dysbiosis

Author Bio
-
Constipation and Motility - always address first before doing any gut or detox work.
-
Support Modes of dysfunction
Adrenals, ammonia, histamine, Liver, oxalates, inflammation, discussed earlier.
-
Finally the Gut Stuff → Broad overview of Biome intervention
Tackle SIBO if present
Look out for high Akkermansia → inflammation
Know what elevated Prevotella likely means
Use Prebiotics + Probiotics + Herbals for your specifics
Assume there is a fungal issue, it doesn’t matter to specify it, you will treat it the same.
1) Support Motility! Tenet #1 might actually not apply to your situation but it must always be screened for and we must always assume that motility issues can develop particularly during the initial stages of intervention. Mitochondrial dysfunction is known to play a role in ASD, the inherent toxic load affects motility and intervention can release more short term toxicity which can exacerbate constipation. One of the worst things clinically is not being able to empty the bowels as it creates a situation where toxicity can not be removed and has the potential to be somewhat reabsorbed.
There are only three ways (maybe a fourth if you are considering exhaling) to eliminate toxicity from your body, this is through defecating, urination, or sweating. Defecating (aka) pooping is a primary mode, if not the primary mode of excreting toxicity. There are classes of individuals (a large number of them in the realm of ASD) where constipation is a daily challenge and often a serious and significant issue. Some individuals in extreme situations do not have bowel movements for days, others require daily enemas and even hospitalization. Although these are the more extreme cases, I firmly believe that we learn the most at the fringes of health. Your intestines function to move fecal matter through a process called peristalsis. The intestines are driven by muscles and those are prone to the effects of brewed/fermenting toxicity, its mitochondria become affected (mitochondrial dysfunction), and motility is slowed. Obviously it is more complicated than this but the point is that before starting any intervention we must do all we can to improve and support motility. We must also realize that when starting any intervention, there is also the potential to impact motility negativity, anything that draws toxicity out of the body will likely do so by dumping into the bowels. Even a topical lotion that increases your glutathione can cause constipation and more toxicity is conjugated and drawn into the bowels. Detoxification is a triple edged sword (three phases) and affects the microbiome. This is my opinion why dysbiosis is for some more perpetual and stubborn than others, because there is a continuing war/burden of toxicity elsewhere in the body that imparts its way into the microbiome as you detoxify.
Something that isn’t talked about enough is the weakness in certain muscle groups, the core, the abdomen and in ASD that also perpetuate motility issues. I would suggest taking a look at abdominal exercises, there are some simple things such as laying your child on their back and having them sit up, using a trampoline, providing appropriate posture and leg support during bowel movements, and regular exercise that can support those muscle modes and help to keep bowels moving. I have suggested these to several individuals in severe motility places and they all have said these exercises have helped in some way. You can find many on youtube for example.
It is well known that just by supporting motility in those when this is a feature, improvement in symptoms can be quite significant. Your body is designed to save water from the stool that enters the rectum as a method to prevent dehydration, this is one of many points where you can re-absorb toxicity that may be present in what your body is trying to excrete. Small intestinal overgrowth “SIBO” also has the potential to affect motility..
In my experience, the best tools that I have come across for supporting motility are:
Fennel Seed, Flaxseed (I prefer powder), Prune Juice, Bifidobacterium Lactis Animals (many use HN019)
L reuteri DSM 17938 although I don’t like to use it upfront to mitigate reaction and reactivity.
Forms of Magnesium, Use of PHGG (gentle up front), Ginger, B6, 5HTP, L-carnitine, Vitamin C, Chamomile, Prune Juice, Cascara, (Senna can be aggravating to the colon). Lactobacillus casei Shirota is also helpful for initiating motility.
You may need to use some or all of these in the most extreme cases. We have formulated Motility Max from Researched Elements largely based on the list above.
Keep in mind that as you start to shift the biome - shedding of bacteria can release toxicity - LPS, cause inflammation and immune reaction, all of which can worsen motility.
2) Support body, metabolism, and other dysfunctions that can often be inferred from symptoms.
A nutritional multi-vitamin (there are many) that provides broad support for the body’s enzyme processes, methylation, detoxification which should include support for mitochondria, the liver, and mineral replacement.
We have developed Spectrum Max to provide the broadest and most complete formulas specific for this purpose. It is important to understand the differences between active and non-active vitamins and that both have utility (Not only the active forms!).
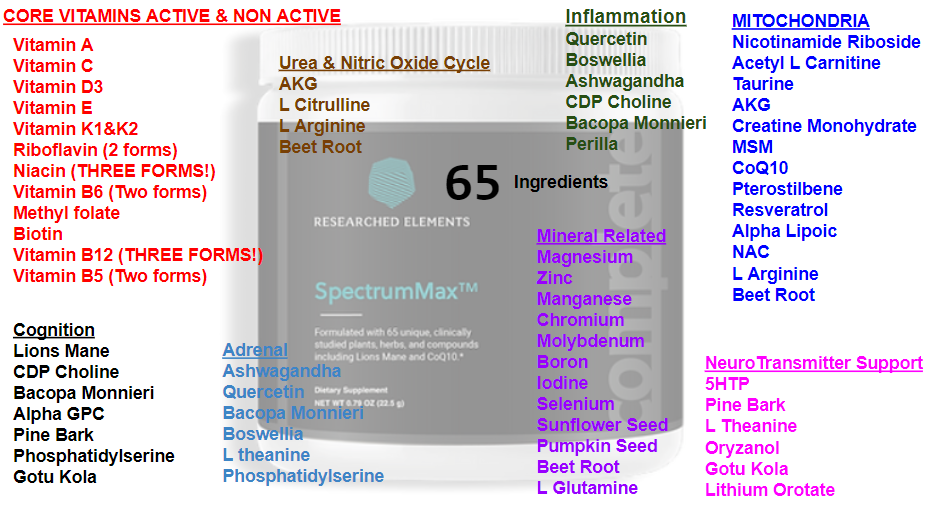
Assessment for the need for Urea/Nitric Oxide Cycle support, this cycle is often taxed and exacerbated by fungal and bacterial overgrowths. Lingering Ammonia can further the dysbiosis narrative. Burden in this area follows with behavior of excessive uncontrollable laughter, night waking, teeth grinding, head pressing, we have developed a product for this called Ammonia Away.
Assessment for the need for oxalate support, exacerbated by fungal overgrowths. Typically associated with symptoms of urinary discomfort, poking at privates or eyes, excessive urination, wetting themselves. We have developed a product for this called Oxalate Relief.
Assessment for the need for MCAS - histamine quelling support, exacerbated by bacterial / fungal, and situations involving mycotoxins and mold. Can be characterized by flairs, reaction reactivity to smells / perfumes, heat intolerance, among others. We have developed a product for this called Histamine Reprieve.
Assessment for the need of adrenal support, typically associated with fear of places, sensitivity to sounds. Often significantly noticeable during chelative-like therapies.
Assessment for liver support - components like milk thistle and related compound or PPC can be integral for some. Reducing the ammonia burden can also be extremely helpful.
You can certainly test for the conditions above but they can be costly and can at times even miss the issue based on the time dependent nature of these dysfunctions. For instance elevations in ammonia are not always constant, they peak and can vary with the digestive cycle and can also be the product of quorum sensing in fungal issues. Many times individuals have measured both high and normal levels in the same day. Know that some tests are better serving to rule things IN than to rule things OUT. Elevations in ammonia present with symptoms of teeth grinding, head pressing, night waking and also carry on to disturb or overload the processing of nitrogen (nitric oxide cycle) and then display as episodes of uncontrollable giddy laughter some of which may characterize as gelastic seizures (it's actually a building up of nitric oxide in the blood which is laughing gas). The issues surrounding ammonia overload can be the product of, bacterial dysbiosis, fungal dysbiosis, parasitic dysbiosis, and even what we believe to be recent evidence of chronic cyanide buildup due to dysbiosis which can convert to ammonia through reaction or bacteria degradation.
Elevated oxalates are the dominant product of fungal overgrowth as we have measured their increase in the wake of antifungal therapy, where the contribution of dietary oxalates pales by orders of magnitude to these fungal oxalate accumulation. Symptoms often present as issues with urination, grabbing of privates, and even eye poking or eye discomfort. The increase in measured oxalic acid can be 4 to 10 times in the wake of an antifungal agent.
As an aide I find that sodium butyrate is the most helpful form of butyrate specifically in ASD, it has been found to assist with reducing ammonia systemically but it can improve immune function through macrophages and even assist with the burden of LPS. Likely the sodium itself plays a role we’ve yet to understand. The most difficult feature of sodium butyrate is its distinct unpalatable odor. We have designed a combination product aimed to assist the mucosa and more called Mucosa & Mind, which includes a substantial dose of sodium butyrate into a great tasting powder at researchedelements.com (available soon).
We have designed specific products at www.researchedelements.com for many of these issues - Ammonia Away, Oxalate Relief, Histamine Reprieve, Motility Max, Spectrum Max, Gut Guardian, Prebiotic Repair, Mucosa & Mind however you can also look to other products on the market to address them. Without supporting these issues, the practicality and feasibility of intervention is reduced.
3) Broad Overview of Biome Intervention
The suggestions that I provide for those that have participated in “Gut Balancing” often fall into the categories below. The suggestions typically include a broad and redundant approach:
- approximately 5 to 15 herbal like components specific to overgrowths
- 2 to 3 primary prebiotic components some specific to deficits in the profile
- 2 to 4 probiotic components. Some are from my foodsforgut.com line, others are specific brands that I have comfort and experience using
- 1 to 3 antifungal directed components
- A gentle biofilm enzyme
- Support for the various modes listed above (histamine, liver, oxalates, ammonia, adrenals, etc.).
There are some items that are included in every set of suggestions (like cold brewed concentrated chamomile Tea)
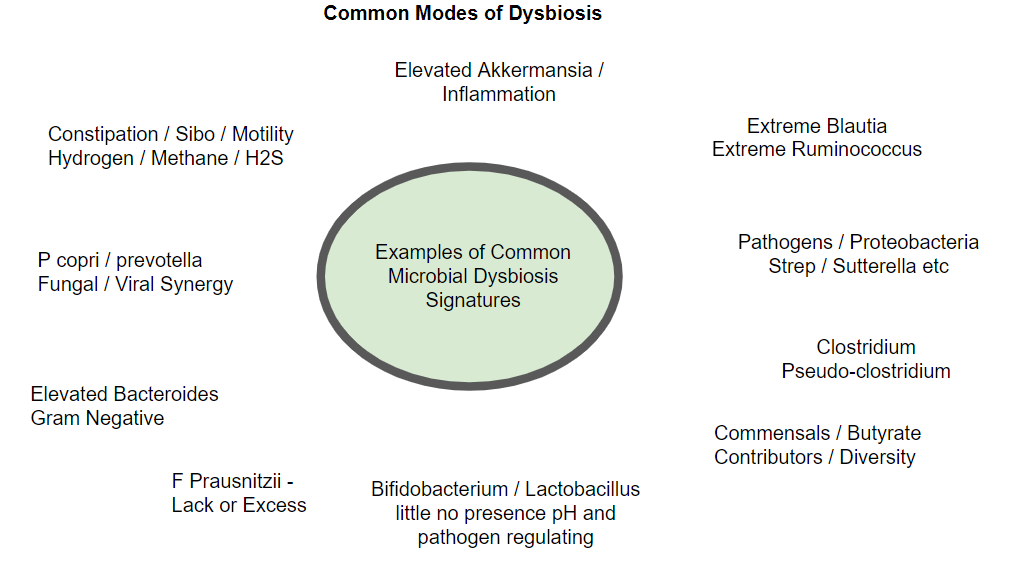
I have listed these common modes as I characterize them in the order that I would tackle them, in some cases it is very important that the order is followed (in terms of their importance as an issue). The way that I do this is by generating suggestions for a 6 week period that increase and change over that duration. Some general principles are and have been already stated.
ALWAYS make sure motility is moving before starting anything - you may need several weeks of pre-treatment.
Address any SIBO components upfront before increasing prebiotics significantly.
Address potential inflammation if observed (Akkermansia significantly elevated);
Prebiotics general ramp up over the first three weeks.
PHGG can be started up front and increased in the second week.
I always include PHGG in every profile unless in some unusual circumstance 1-3 tablespoons daily, it is always safer to start slower and ramp up.
PHGG is appropriate and helpful in all forms of SIBO and should be used (slowly) in conjunction with other tools.
GOS can sometimes be started upfront if needed however I delay its use in cases of certain SIBO.
GOS is used for every profile that requires bolstering of Bifidobacterium.
GOS is particularly appropriate for overgrowth of Desulfovibrio.
My selection of potential prebiotic tools that I limit myself to are (Lactulose, Glucomannan, PHGG, GOS, artichoke (rarely pure inulin), apple pectin, acacia fiber). I do not use XOS, FOS and have stopped using HMO, very rarely will I resort to inulin. Researched Elements has a prebiotic blend designed to provide the middle of the road feeding and diversity enhancement as you use other tools like Gut Guardian in your dysbiosis regimen. Glucomannan is often a 1st tool to assist with Lactobacillus (be careful of choking hazard), next apple pectin can assist here. Consider adding less reactive cheeses such as Goat's cheese (feta is a type of Goat / Sheep milk cheese) which can help to bolster this genus. Acacia is my second choice to bolster Bifidobacteria, lactulose can be an invaluable all around tool even with the fungal territory and is especially helpful in reducing overgrowth in Bacteroides, it must be used with oversight, slowly and you need to rule out SIBO components before use. Although Lactulose can be an immensely helpful tool with elevated Bacteroides, I however had much success with high dose polyphenols in this area too.
I always include a low dose of caprylic acid for antifungal support, (taste is very palatable which is always a big consideration in ASD and children), and it is an efficient fuel to support mitochondria. When possible I like the use of undecylenic acid, the taste is unbearable for those that can not swallow. You might do better with Megamycobalance from microbiome labs as they provide smaller capsules and include Bee Propolis but your child likely needs to swallow capsules first unless you are a master at disguising taste.
I sometimes include homeopathic antifungal components that bolster the immune response, these include pekana mucan, or polyfungal, or other homeopathics in this realm. (Caution here requires practitioner oversight). Oftentimes I may consider these during a second or third round of intervention.
I sometimes use Pau D’arco and Laterosporus BOD to assist fungal situations. Remember you should assume there is a fungal issue and cover it with a minimum of caprylic acid and a light biofilm enzyme such as candex. Symptoms or other markers can give you insight to the extent of the fungal issue. I do not recommend using prescriptives like Nystatin or Diflucan or Itraconazole especially upfront. I reserve the possibility to entertain them only later on and after attempting microbial balancing. I don’t believe they are necessary or better than most of the non-prescriptive tools we have, if they are used, one should consider pulsing them. I will actually discontinue working with individuals that use these actively during balancing suggestions as it makes the balancing nearly impossible to compensate for at times.
Probiotics increase over the 6 week period specific to the profile, typically I select from
AZ1, AZ2, Thorne Bacillus Coagulans, Klaire S Boulardii, L johnsonii, BB536, HN019, DSM17938 where appropriate. I typically do not like giving probiotics every day at first, and will start with every other day.
Introduce a light biofilm enzyme (I prefer Candex) in the 3rd to 4th week, be cognizant of oxalate and ammonia issues. I typically suggest this every other day.
Retest at the end of 6th week and damp down suggestions until new results are ready. Rinse and Repeat for at least three rounds.
Some more comments on the probiotics that I use
AZ1 is a blend made for me by foodsforgut.com and I use it for broad bacterial dysbiosis.
AZ2 is a blend made for me by foodsforgut.com and I use it for antifungal activity.
These products are not sold by me nor do I receive any royalties for them, they are simply formulas that I have devised and foodsforguts.com has offered to sell.
Klaire Labs S. boulardii is the best S. boulardii that I have encountered and I have used it for years and in hundreds of individuals alongside the dozen or so practitioners that receive my suggestions. I use S. Boulardii when there are elevations in clostridium and pseudo clostridiums (clostridiums renamed to other genus and other bearing the clostridium postfix). There are a lot of concerns about S. Boulardii, know that there has been historical confusion between S. cerevisiae Boulardii and S. cerevisiae, a true S. Boulardii is transient and does not colonize. The only other S. Boulardii that I like and use is by Florastor. S boulardii won’t cover all these clostridium / pseudo-clostridum issues but it is a great place to start.
I use bacillus coagulans to effectively fix deficits in underpopulation of F. prausnitzii.
I use L reuteri Dsm17938 to assist in Methane and Hydrogen SIBO situations alongside other components.
I sometimes will use BB536 and Plantarum 299V however I found that other less popular strains can also do the job and for less expensive prices.
I do not use akkermansia (dead or alive) as I have found it pointless and providing limited transient benefit if any.
I have recommended in the past Visbiome, I believe it to be a good product.
I have used in the past laterosporus BOD to assist with certain fungal issues.
I have used Miyarsian, Clostridium Butyricum in the past and I find it helpful in some with IBS.
I have used SilverFern Brand probiotics which I find a better variant of Megaspore however I have stopped using these commonly and will only resort to them if other situations have failed. Typically I might call on them for situations of extreme proteobacteria, this is rare.
More on Biome Specific Situations - Disclaimer
- Always speak with your practitioner before use.
- I have only outlined some modes of imbalance.
- Many will believe that species level scrutiny is necessary. I have found that targeting at the genus level is often sufficient.
Elevated Akkermansia: A sign of inflammation potentially local in the intestines and will reduce in the presence of anti-inflammatory compounds like Curcumin / Boswellia (there are others). Typically following the administration of these anti inflammatories extreme akkermansia levels will drop to near zero quickly. Mucus secretion can be driven by a local inflammation that may be artificially driving akkermansia at that specific point, giving the false impression of the health of the mucosa. I would generally say that anything over 6-8% abundance is potentially indicating pockets of local inflammation feeding akkermansia (mucus).
Depleted Akkermansia: Not high on my list of concerns. This is something that comes at the tail of healing and is a surrogate for intestinal permeability / damaged mucosa. Akkermansia is a mucin-feeding microbe, restoring the mucosa takes time and is key to replenishing this. Researched Elements has a product in development called Mucosa and Mind which will be out Late December 2023. I don’t find sustained utility in taking dead or alive Akkermansia however I’m open to its use.
Assess for SIBO symptoms via comprehensive questionnaire, combined with evaluations of methane dominant microbes like Methanobrevibacter, assess for overgrowths in dominant H2S producing microbes. Understand that hydrogen is required for Methane (CH4) and Hydrogen Sulfide (H2S), assume the potential for Hydrogen SIBO to be at play. Understand that Bilophila overgrowths can mean the body is attempting to produce more bile to increase detoxification.
Methane, Methanogens: Fennel seed, Green Tea extract, Cinnamon, Guava Leaf, L Reuteri-DSM17938 although I have used other reuteri strains with success. I always like to support these SIBO signatures with HN019 B lactis. I do not like to use herbals like Thyme or Oregano, I believe they are too strong and counterproductive.
Other tag on options for stubborn SIBO situations include sodium butyrate, colostrum, bee propolis.
Always make sure to emphasize red / purple based polyphenols alongside the above, these include Cranberry, bilberry, acai, dragon fruit, beet root, wolfberry, these polyphenols are great for SIBO overgrowths of all types and helpful in IBS / IBD. I particularly stay away from herbs like oregano or thyme due to their impractical taste and their potential for knocking out beneficial microbes. I always include olive leaf because of its systemic action, broad targeting of bacteria, fungi, virus, neuroprotective components, and I have not seen it have negative effects on the biome.
H2S - Desulfovibrio - codonopsis, cranberry (polyphenols), L plantarum, GOS,
H2S - Bilophila (it's important to understand that elevations here can actually be the product of upregulated bile flow as a mechanism to bolster detoxification). Cranberry, L plantarum, Chamomile, L Paracasei, HN019, Fennel, Codonopsis
Include broad coverage for Hydrogen when other SIBO modes are present, I prefer colostrum, goldenseal, L reuteri, S boulardii, and support for motility.
Lack of F prausnitzii - if so support with Bacillus Coagulans. I typically use Thorne, however I’m not a fan of the titanium dioxide.
Elevations in L Rogosae i have found the combination of curcumin and goldenseal to be helpful.
I prefer to use GOS initially over acacia fiber for bifidobacteria as I find that acacia can further fuel an already existing overgrowth of L Rogosae, at the same time I will mix GOS with curcumin / goldenseal when this is overgrown. I find that these overgrowths sometimes correlate with OCD type behaviors.
Lack of or diminished Bifidobacterium - Primary emphasis on GOS. I do not like using HMO. I find it to be somewhat unpredictable in its outcomes. Build in Acacia Fiber if/as needed. Other herbs have a supportive role, codonopsis, ginger.
Lack of True Lactobacillus
Glucomannan, then apple pectin. Do not use it on a daily basis, be aware of overdosing on large amounts of Glucomannan there is potential for asphyxia, better to introduce small doses.
Elevations in Clostridium or Pseudo Clostridium which include assessment of the following genus
Lachnochlostridium, RuminiClostridium Erysipelatoclostridium and other genus that have clostridium species names that have been reallocated to other genus, (Etnerocloster, Thomasclavelia, Anaerotignum, Oscillospiraceae incertae sedis, Anaerotignum, Hathewaya, Tyzzerella, Mediterraneibacter.
The main tool that I use is Klaire Labs S Boulardii, and possible addition of Florastor S boulardii. Klaire has the most effective S boulardii. The therapeutic dose depends on the elevations, effectiveness is not the same for all these genus. I find you may need to reach 5 to 6 capsules daily for an extended period of time. I find that colostrum, L Rhamnosus GG helps.
Elevations in Prevotella: Both fungal and viral implicated. Prevotella overgrowths occupying double digits certainly align with fungally fed situations. Best tools for these overgrowths.
Codonopsis/Ashwagandha, Perilla, Vitamin A, Bacopa, Boswellia, Olive leaf, L Johnsonii, Rosemary, Curcumin, Ginger. Also Introducing antifungal components. AZ2 probiotic and support for fungal overgrowth which can include. A light biofilm enzyme given on alternative days like candex for the 6 week duration at least.
Elevations of Bacteroides: High dosing of red and purple polyphenols, acai, bilberry, cranberry, beetroot, raspberry, dragon fruit, Pomegranate wolf berry, green tea, codonopsis, acai. Lactulose is very effective at reducing Bacteroides but must be used with caution, in general lactulose is a very helpful tool for repairing the gut but one needs to rule out motility / SIBO issues before using and it must be used slowly.
Elevations in Proteobacteria: I find that pomegranate peel (husk or hull) to be very effective here. I find that when needed additional bolstering can be provided by colostrum (I use the Sovereign Brand) alongside AZ1 probiotic, profile appropriate prebiotics, Guava leaf, B subtilis, L Reuteri, BB536, L Rhamnosus GG.
Elevations in specifically Sutterella & Parasutterella: L Paracasei, DGL (AZ1)
Of which some specifics include
Elevations in Streptococcus: Pomegranate Peel, Colostrum
Elevations in Blautia: L paracasei, Cranberry, Red Polyphenols, Triphala
Elevations in Ruminococcus: L paracasei, Flaxseed powder, Cinnamon, Olive leaf, Triphala
Elevations in Tyzzerella: High dose red polyphenols, Green tea, Flaxseed Powder
Elevations in F Prausnitzii: Flaxseed powder, L Paracasei
Elevations in Fusobacteria, Rosemary , Cinnamon, Bacopa, Green Tea
Elevations in Eubacterium: Flaxseed powder, Ginger
Elevations in Lachnospira: L Paracasei, L Reuteri
Best tools for the mucosa
High dose red/purple polyphenols
Addition of cruciferous veggies - assists with Glucosinolates and Glutathione in Colon
Keep inflammation down
Introduction of glutamine components at a later stage when it is does not cause excitability
Most Common Components to include that seem to provide benefits in most regardless of profile
Concentrated Cold brewed Chamomile Tea, Codonopsis, Bacopa, Olive Leaf, Beetroot, PHGG, GOS
Concerns about H Pylori
Chamomile, L Reuteri, Triphala, Codonopsis, Ginger, Fennel, Curcumin
Herbs or Compounds that assist with Glutamate Regulation
Curcumin, Bacopa, Boswellia, Codonopsis, Ginger, Pterostilbene, Acetyl L Carnitine
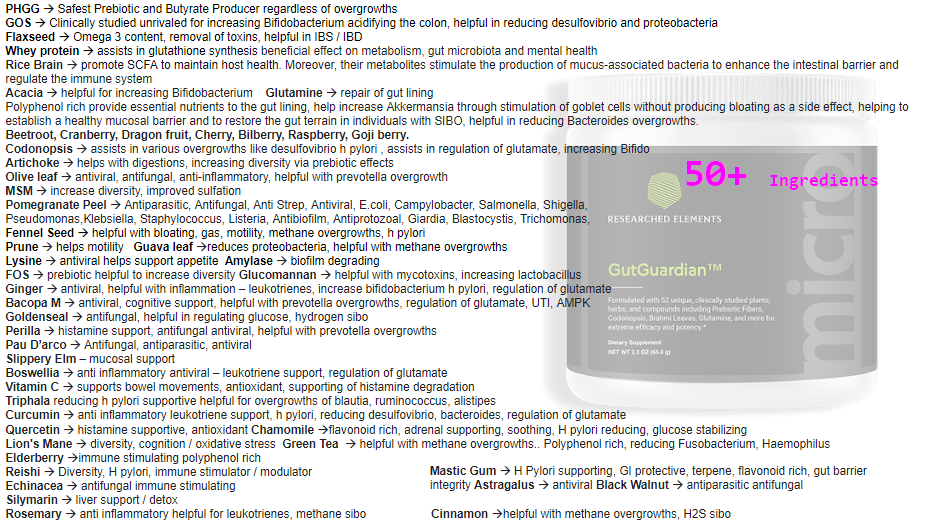
If you are having a hard time starting due to difficult of finding a practitioner or being overwhelmed with the complexity of your problem, please give a look at Gut Guardian which we designed to be a core tool to navigate dysbiosis.
Categories: dysbiosis treatment guide Tags: dysbiosis treatment guide